For Patient Information
We deal with wide variety of issues related to spinal & orthopeadic complains. This section provides some general information about variety of spinal and orthopedic issues.

Acute Back Pain
It is pain in the back, anywhere between the lower ribs and the buttock crease. It is simply an episode that is shorter than 6 weeks in duration. It can be very painful and very frightening. Fortunately, it most commonly gets better on its own. What most patients seek from doctors is how to get better quicker and how to reduce the chances of it happening again. Acute back pain is common. 80% of people experience back pain during their lifetime and as many as 50% of the population will have an episode of back pain in any one year.
Some Indicators includes previous diagnosis of cancer, unexplained weight loss, pain that continues to get worse despite good pain killers, pain that wakes you from sleep at night and a first episode of severe back pain over the age of 55 years.
Treatment in which Physiotherapy, chiropractic and osteopathic treatments do not seem to have a large effect in the first 4 weeks of an acute back pain episode. This is because it so often gets better on its own. The role of health care professionals is mainly around giving the ‘right’ message and the reassurance that there is nothing seriously amiss. Avoiding ‘mixed messages’, which can be very confusing is important, so make sure you use reliable information sources that hopefully are not too ‘commercial’.
Nerve Root Pain
Nerve root pain comes from a nerve in the spine. Nerves carry messages about sensations and control of muscles and so disorders of nerves can cause pain, numbness, increased sensitivity or weakness of muscles. The pain is often felt in the area of the body supplied by that nerve. It is common for the leg nerves and arm nerves to be affected.
Lumbar nerve pain (often called ‘sciatica’) generally goes below the knee. Back pain is usually felt between the lower ribs and the buttocks. Often there will be a combination of back and leg pains.
Brachial neuralgia (nerve pain in the arm) comes from the neck nerves. Sometimes the pain goes down the arm as far as a specific finger.
Radicular pain is a term doctors use to describe pain when it is mainly from a single nerve root


Scoliosis
Scoliosis simply means a lateral deviation of the spine. It is usually detected in childhood. Some patients may have an underlying disorder that is associated with scoliosis such as muscle weakness or imbalance. Idiopathic scoliosis is a curvature of the spine that doesn’t appear to be due to any other medical condition. Current research suggests that it is mainly genetic in nature.
Some Causes may include when the rapid growth around the time of puberty occurs. If the cause of the scoliosis is not known it is called ‘idiopathic’. At present there is some evidence that there is a genetic component to it and there is a family history in some cases. Identical twins have identical curves usually.
Its Occurrence varies from different age groups.In children that present under the age of 6 it is called early onset. When it occurs in the very young, it can sometimes progress and be a serious disorder. It is most common in teenagers and is usually a cosmetic issue, so some patients may be unconcerned and some may be bothered by the appearance of their spine. It is not a weakness of the spine and it isn’t usually painful. Scoliosis in Adults can arise as a result of the ageing process, if it first appears in later life it is sometimes called ‘de novo’ scoliosis.
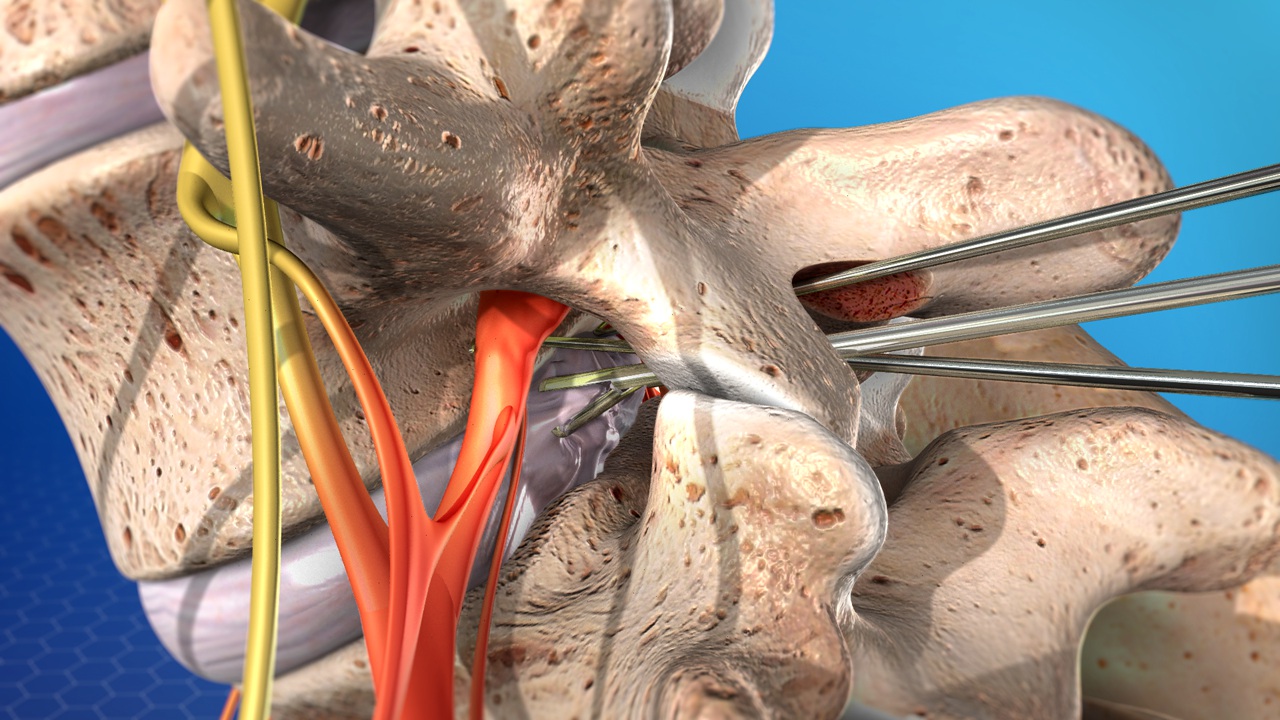
Lumbar Disectomy
A discectomy is carried out to release the pressure on your spinal nerves caused by a bulging or slipped disc. As with a laminectomy, the surgeon will make an incision over the affected area of your spine down to the lamina.
Usual Benefits include 70-75% of patients experience a significant improvement in leg pain. 20-25% may be better but still have persistent leg pain. 5% may have no benefit at all. 1% may be worse in terms of pain.
Some Considerations are important for patients. Spinal surgery for sciatica and spinal stenosis is better for the leg pain than it is for back pain but both pains may improve. Symptoms of numbness or weakness may well persist after surgery. In patients attending general practice for the first time with sciatica, 75% are better within 28 days. Surgery for disc prolapse has a recurrence rate of between 7% and 15% within ten years. This is the same whether or not you have an operation. Surgery has less risk and is safer on fit and healthy patients. Some pracautionary measures such as stopping smoking, loosing weight and improving aerobic fitness all help. Older patients may have specific risk factors such as heart disease. Tablets used to thin the blood increase the risks of bleeding and you must inform your surgical team regarding these. Patients who are diabetic have a slightly increased risk of infection generally and the nerves in diabetic patients may not recover as well as others. Specific risk factors may apply to you as an individual.
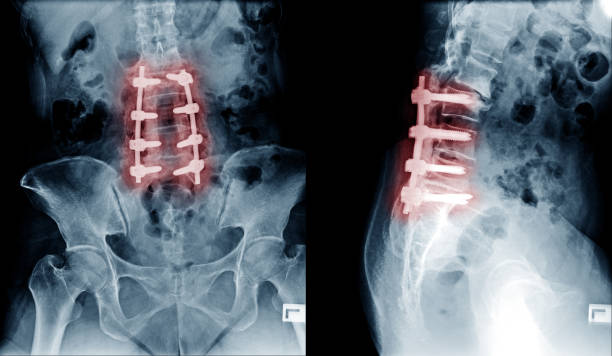
Lumbar Spine Decompression
The operation of lumbar decompression seems to improve pain in about 65-70% of patients and often improves the distance a patient can walk by a factor of about four. The operations are for quality of life issues. That is, if the symptoms are acceptable to the patient the question of having surgery or not having surgery should be made by patient in discussion with the surgeon. The operation is usually done under general anaesthetic and involves a short hospital day, quite often just overnight. Most surgeons encourage an early return to normal activities as that helps people to get better quicker.
Risks of Surgical Treatment are not general. They vary from patient to patient and their situation. Some of the risks include: The risk of paralysis, which means loss of use of the legs, loss of sensation and loss of control of bowels and bladder is low. Probably occurring less than one per 300 operations. Superficial wound infections are not rare and may occur in between 2% and 4% of spinal operations. Risks of infection are increased in diabetic patients, patients on steroids or those with lowered resistance to infection. The spinal nerve causing the pain may be already damaged by the disease process. The disc prolapse can cause scarring with in the nerve such that it is unable to recover despite technically successful surgery. Damage to the main blood vessels at the front of the spine (the aorta) has been known to occur bt its occurrence is less than 1 per 10000 operation.
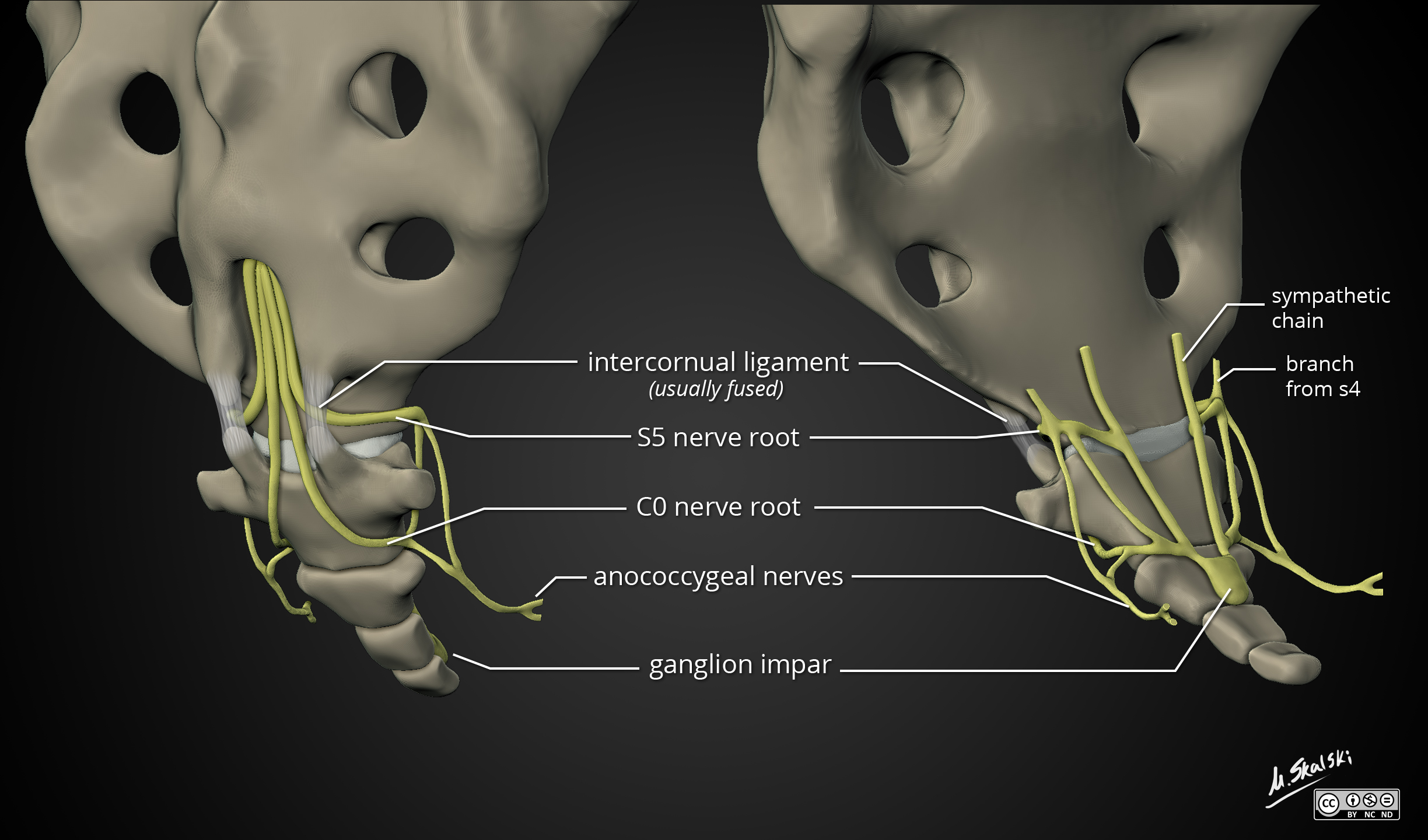
Coccydinia and Operations for Coccygeal Pain
It’s a collection of conditions which result in pain in the area of the coccyx (tailbone).
Common Causes of coccydinia are poorly understood and there are numerous theories proposed for its origin. Some of the major causes are a fall on the buttocks, accidents like slipping while wlaking down stairs, or a fall when skating and disposition of joints during pregnancy. Other common causes include nerve pain secondary to repeated damage, cyst formation, infection, lump around the region, obesity and a bursitis like condition that can arise in slip patients.
The Diagnosis is almost clinical. The main purpose of visiting the doctor is to rule out other causes that have been discussed above. Various X-rays help greatly in diagnosis or assist in managing the problem. Further special tests like MRI and Bone scans are only done in rare situations when the diagnosis is in doubt or other causes are being rules out.
The Treatment might take weeks or months of conservative treatment before significant pain relief is felt. If there is persistence of symptoms, the doctor might offer an injection. This is usually at the joint (sacro-coccygeal) which is thought to generate the pain. Physiotherapy and Manipulation of Coccyx are not so much helpful. Surgery in the form of coccygectomy is usually the last resort. Various case series have shown about 60-70% good or excellent results on a carefully selected group of patients.